Oropharynx
Anatomy
The oropharynx is the central most region of the pharynx, extending from inferior to the nasopharynx to the hypopharynx. The oropharynx contains the soft palate, palatine tonsils and base of tongue. Within these regions are additional structures:
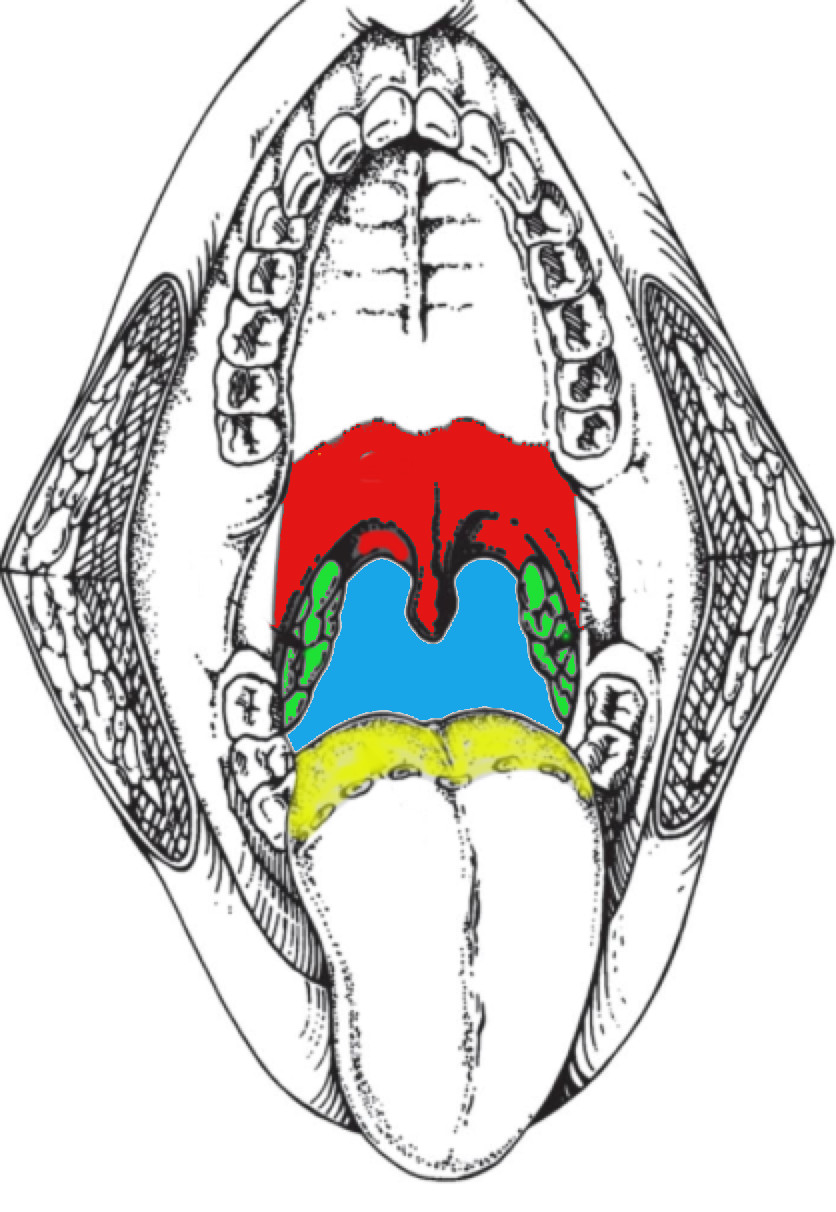 |
| palate (RED) with anterior and posterior pillars surrounding the palatine tonsils. |
| Palatine Tonsils (GREEN) between the pillars. |
| Base of Tongue (YELLOW) |
- Soft Palate
- The soft palate separates the nasopharynx from the oropharynx. It is posterior to the hard palate and extends to and is contiguous with both the anterior and posterior tonsillar pillars. All tissue anterior to the soft palate is considered oral cavity. No part of the soft palate is considered nasopharynx, although it provides the floor of the nasopharynx. Most tumors of the soft palate arise from the oropharynx aspect.
- Palatine Tonsil
- These are located poserio-laterally on the lateral wall of the oropharynx. The tonsillar fossa encases the tonsil and is bounded by the anterior and posterior pillars. These pillars contain the palatoglossus and palatophyaryngeus muscles. They join with the soft palate.
- Anterior pillar (anterior faucial arch)
- Posterior pillar (posterior faucial arch)
- Pharyngeal wall
- The posterior pharyngeal wall is bounded and continguous with the inferior aspect of the nasopharynx at the level of the soft palate. The wall extends laterally and anteriorly to make up the posterio-lateral aspect of the oropharynx. In consists of the pharyngeal constructor muscles and the overlying mucosa. It continues inferiorly to the level of the hypopharynx.
Lymphatics
The primary drainage is to the Level II nodes. The tonsils, lateral soft palate, base of tongue and lateral and posterior pharyngeal walls also drain via Level VII (retropharyngeal) nodes. Level III/IV and V usually occur after other nodes are involved (Level II). The RP Level VII nodes are involved if BOT, lateral pharyngeal wall, and are mostly to the lateral RP nodes (Level VIIb, I think). Involvement of the medial RP nodes is rare. Level I and V nodes were nearly always associated with involved nodes in Levels II-IV.
Studies have been done to determine the extent of retropharyngeal nodal involvement. Hasagawa found in a 1994 surgical series of hypopharynx and oropharynx cancers that 50% had positive RP nodes, with 20% in the pN0 group and 64% in the pN+ group. Nasopharyngeal cancers were the highest RP involvement at 79%, followed by pharyngeal wall involvement.
Pathology
Most are squamous cell cancers. Tonsilar cancers have a higher percentage of HPV positive disease (p16 positive).
Natural History
Soft palate grows by direct extension and nodal metastases. Tumors are almost exclusively found on the oral cavity aspect, rather than the NP aspect. They can extend to involve the pharyngeal walls and tonsils. Occasionally they extend superiorly into the nasopharynx. Lesions that approach the midline tend to spread to the bilateral and retropharyngeal nodes. These tumors can spread to the tonsil, pharyngeal wall and base of tongue. They can track the palatine nerve to the base of skull.
Tonsil cancers can spread to the buccal mucosa, retromolar trigone and base of tongue. In well lateralized tumors, ipsilateral Level II/III nodes are at highest risk. 60% of tonsil cancers involve the soft palate (Perez), and half involve the BOT
BOT cancers are insidious, frequently appearing as neck metastases well before clinically apparent BOT disease is seen. Later stage BOT cancers result in nerve involvement with fixation of the tongue, extension into the oral tongue and down to the vallecula and epiglottis. Disease can also extend laterally to the pharyngeal walls. Disease frequently involves the Level II nodes, followed by Level III and is bilateral. 70% have ipsilateral nodes, 25% have bilateral nodes.